
Abstract
Ankle sprains are very common injuries and are usually managed non-operatively. With poor rehabilitation, 20% of ankle sprains may develop chronic instability, which often necessitates surgical intervention. Rehabilitation after such procedures is focused on regaining the function of the ankle while keeping a stable joint. Post-operative rehabilitation and weight-bearing status varies greatly among surgeons. Our aim is to review the existing most recent literature that investigates post-operative outcomes following different rehabilitation protocols in patients with Chronic Lateral Ankle Instability (CLAI).
We performed a literature search from 2002 to 2022, through Medline/Pubmed databases using the terms ‘ankle lateral ligament’, ‘repair’, ‘reconstruction’ and ‘post-operative rehabilitation’. A gray literature search was also performed using the Google Scholar search engine. Studies that described post-operative rehabilitation protocols following CLAI surgery were included.
25 studies with 1045 patients describing rehabilitation protocols following repair/reconstruction of CLAI were included. Most studies used the Broström procedure or modification of it. In 82% of cases patients were immobilised in a cast from day 1 post-operatively for two weeks and were kept non-weight-bearing in 64% during the same time. A boot or brace was kept up to 6 weeks in 82%. Full weight-bearing was recommended either at the very start following surgery (32%), or after four weeks from surgery (36%). Early range of movement exercises started after week 2, with muscle strengthening, proprioception, and balance between week 2 and 6. Return to sports is usually between 2-4 months.
In conclusion, post-operative rehabilitation protocols following CLAI surgery vary considerably. We attempted to quantify the studies that provide enough information on this subject and create a post-operative rehabilitation protocol following anatomic repair/reconstruction for CLAI.
Keywords: Chronic lateral ankle instability; Modified broström-gould; Post-operative rehabilitation
Introduction
Emergency Departments are inundated with musculoskeletal trauma, with up to 50% resulting from ligamentous injuries [1]. Amongst these, 40% involve the ankle, the lateral ankle ligamentous complex injuries being the most prevalent within the sporting community and the general population [2]. The Anterior Talofibular (ATFL) and Calcaneofibular Ligaments (CFL) are the ones that are most commonly injured [2]. Management of these ankle sprains is mostly conservative, but it is reported that, with poor rehabilitation, up to 20% can result in chronic instability [3]. This may manifest as frequent ‘giving-way’ of the ankle while weightbearing, or inability to return to sports due to the lack of objective stability, for more than 6 weeks from injury. While most acute ankle sprains can be managed conservatively, Chronic Lateral Ankle Instability (CLAI) may require operative management, when conservative measures fail [3,4].
Nonoperative management is the initial approach for treating CLAI, with physiotherapy, orthotic devices, and proprioceptive training. However, in persistent instability or failure of conservative measures for more than 3 to 6 months, operative management can be considered [5]; this includes anatomic ligament repair or reconstruction and non-anatomic reconstruction techniques [6]. The Broström technique, first described in 1966, offers anatomic repair of the ATFL and CFL, and is considered the gold standard [2]. There have been many modifications to this technique, as well as arthroscopic variants [5].
The recovery period after such procedure is between 3 and 6 months [2]. Rehabilitation protocols are essential to allow for patients to regain their range of motion in the ankle [5]. However, the optimum length of rehabilitation as well as the main concept of early versus late mobilization is still controversial [5]. Some surgeons are protective of the repair/reconstruction and keep ankles immobilized in a cast for up to 6 weeks. While this protects the repair, it can also lead to decreased ankle motion and muscle atrophy, making the overall rehabilitation process more challenging (and not conducive for a return to sports) [2]. Others allow early mobilization of the ankle, but this also comes with risks of complications, especially wound-related [2]. Confidence in the reconstruction of the ligamentous structures has improved with the use of anchors and polyethylene suture material; however the orthopaedic dogma of postoperative immobilization remains. Our aim was to perform a narrative review of the most recent literature describing postoperative rehabilitation protocols after surgical management of CLAI.
Methods
A literature search was performed via Pubmed/Medline databases using the terms ‘ankle’, ‘lateral collateral ligament’, ‘repair’, ‘reconstruction’ and ‘post-operative rehabilitation’, for studies that investigated different rehabilitation protocols in patients with CLAI from 2002 to 2022. A gray literature search was also performed using the Google Scholar search engine. We felt that a 20-year period is a good representation of the published literature on this subject, given that the number of studies published on CLAI has significantly increased since 2014. Articles included in this review were studies describing their post-operative rehabilitation protocols following CLAI surgery, comparative or case series. If the description was incomplete, or the authors failed to provide timings for the rehabilitation period, the study was excluded.
Protocols were categorized based on the type of surgery: anatomic repair or reconstruction, and non-anatomic reconstruction (Figure 1). We recorded the type and length of immobilization, weight-bearing status and type of exercises allowed with physiotherapy, including time frames, and the complications reported. We lastly looked for aim to return to work and sport. Using the evidence, we attempted to create a standardized rehabilitation protocol based on type of repair/reconstruction performed.

Figure 1: Search strategy (2002-2022) and included studies.
Results
Initial search identified 4554 articles. Following removal of unrelated research, duplicates, and studies not providing enough information on post-operative rehabilitation protocols, we included 25 studies (Figure 1). 22 studies described anatomic repair or reconstruction techniques and 3 studies non-anatomic reconstruction methods. Table 1 shows in detail each study, along with the number of patients included, the surgical technique used, rehabilitation protocol and complications. In the anatomic repair/reconstruction group, there were 929 patients in total, compared to 116 in the non-anatomic reconstruction group. Most studies in the anatomic group described a variation of the Broström procedure, with or without arthroscopy (15/22, 68%). 2 studies used the Karlsson procedure (9%), 4 studies described arthroscopic reconstruction techniques (18%) and 1 study Arthroscopic Lateral Ligament Repair (ALLR) (4.5%). In the non-anatomic group, there were three different techniques described: modified Watson-Jones, fibular periosteal flap, and a split peroneus brevis graft. We looked at the rehabilitation protocols separately for anatomic and non-anatomic reconstruction groups. Specifically, we looked at the type and length of immobilization along with the weight-bearing status. Secondly, the timing of exercises and type of exercises and the overall length of rehabilitation required to return to sporting activities.
![]()
Study
Surgery
Patient N
Immobilization
Weight-bearing*
Physiotherapy (exercises allowed)
Return to sports
Complications (N)
Anatomic Repair / Reconstruction
Teramoto et al (2022) [7]
Arthroscopic Lateral Ligament Repair (ALLR)
22
- Day 0-3: Fibreglass backslab
- Day 4 – Week 3: Ankle brace during day & fibreglass backslab at night
- Day 0-3: Non-WB
- After day 3: FWB
- Day 3 – Week 3: Ankle dorsi-flexion, walking, squats, foot intrinsic muscle training
- Week 3-4: Ankle plantar flexion & dorsi-flexion strengthening
- Week 4: Jogging
- Week 6: Competitive sport training
8 weeks
Not stated
Yang et al (2022) [8]
Arthroscopic vs Open Anatomic Reconstruction
Arthr.: 10
Open: 10
- Week 0-4: Ankle boot
- After week 4: high ankle shoes
- From day 1: partial WB
- From week 4: FWB
- From week 2: ROM exercises
4 months
- Superficial wound infection (1)
- Stitch abscess (1)
- Transient sural paraesthesia (1)
Martin et al (2021) [9]
Open modified Broström
93
- Week 0-2: Cast
- Week 3-4: Walking boot
- After week 4: ankle lace-up brace
- Week 0-2: Partial WB
- Week 2-: WBAT
- Week 2: home resistant band strengthening
- Week 4: stationary biking, water therapy
- Week 4-6: treadmill, elliptical training, proprioception, heel raises
- Week 6: jumping
100 days
- Cellulitis (1)
- SPN# hyperesthesia (2)
Baraza et al (2017) [10]
Open modified Broström-Gould
21
- Week 0-6: Cast
- From week 6: malleolar splint
- Week 0-6: Non-WB
- From week 6: FWB
- From week 6: gentle ROM exercise
Not stated
- Persistent ankle pain requiring re-operation (3)
Jiang et al (2017) [11]
Open modified Broström-Gould +/- Arthroscopy for OCL8
34 (+ arthr.)
36 (- arthr.)Both groups
- Week 0-3: Splint
- Week 4-6: Ankle brace
Group A (+ arthr.)
- Week 0-6: Non-WB
- Week 7-8: Partial WB
- Week 9-12: FWB
Group B (- arthr.)
- Week 0-4: Non-WB
- Week 5-6: FWB
Group A
- Week 2-6: daily full range continuous passive motion, no varus (from week 5) or internal rotation
Group B
- Week 3: daily full range continuous passive motion, no varus (from week 5) or internal rotation
Group A
- 4-6 months
Group B
- 3-4 months
- Continuous ankle instability (6 – 3 each group)
Jeong et al (2016) [12]
Open modified Broström
45
- Week 0-4: Cast
- Week 5-6: Ankle orthosis
- Week 0-6: Non-WB
- From week 6: Partial WB
- From week 4: Gentle ROM exercises
- From week 6: peroneal muscle strengthening + proprioception exercises
- After 3 months: light exercises
Not stated
None
Russo et al (2016) [13]
Open modified Broström-Gould
18
- Day 1: ankle brace
- Day 1-14: very light WB
- From day 15: increasing partial WB
- From day 15: flexion-extension exercises, peroneal muscle strengthening, proprioception
- From 3 months: running
4 months
None
Acevedo et al (2015) [14]
Arthroscopic Broström
93
- Week 0-2: Cast
- Week 3-4: Walking boot
- Week 5-12: lace-up ankle brace
- Week 0-2: Non-WB
- Week 3-4: WB as tolerated
- Week 5-6: FWB
- Week 2-4: gentle ROM avoiding inversion
- Week 4-6: Plantar and dorsi-flexion
- Week 6+: peroneal muscle strengthening, balance, stationary bike, proprioception
3-6 months
- Post-operative neuritis (5)
Cho et al (2015) [15]
Open modified Broström
24
- Week 0-3: Cast
- After week 3: elastic ankle bandage
- Week 0-3: Non-WB
- Week 4: Partial WB
- After week 5: FWB
- From week 3: ROM exercises
- From week 4: peroneal muscle strengthening, proprioception training
- From week 6: running
8 weeks
- SPN damage (1)
- Wound infection (1)
Cho et al (2015) [16]
Open modified Broström
[suture bridge vs. suture anchor repair]45
- Week 0-3: Cast
- After week 3: elastic ankle bandage
- Week 0-3: Non-WB
- Week 4: Partial WB
- After week 5: FWB
- From week 3: ROM exercises
- From week 4: peroneal muscle strengthening, proprioception training
- From week 6: running
3 months
- Wound infection (1)
- Skin irritation (3)
Iawo et al (2014) [17]
Open modified Broström
10
- Week 0-4: Cast
- Week 0-2: Non-WB
- Week 3-4: Partial WB
- From week 5: FWB
- From week 4: ROM (plantar flexion and dorsi-flexion) + muscle strength exercises
- From 2 months: inversion, eversion, balance
- From 3 months: functional training (running, jumping)
Not stated
Not stated
Petrera et al (2014) [18]
Open modified Broström
49
- Day 0 – week 6: Pneumatic walking boot
- From day 0: FWB
- 0-3 weeks: ROM, hip & knee strengthening, limited plantar (0-20°) & dorsi-flexion (0-10°) in NWB mode
- 3-6 weeks: progress with active ROM but avoid inversion
- From 6 weeks: progress ROM and include inversion, proprioception. gait training, swimming, biking
- From 3 months: sports-specific training, running, plyometrics
When full pain-free ankle ROM. >90% ankle strength of contralateral ankle, pass sports-specific tests
- Superficial infection (2)
- SPN paraesthesia (1)
- Residual instability (3)
Buerer et al (2013) [19]
Open modified Broström-Gould
41
- Week 0-4: Cast
- Week 4-8: ankle splint (day + night)
- Week 8-12: ankle splint (only night)
- From day 0: FWB
- From week 5: ankle tonification
- Week 7: proprioception & coordination training
- One plane sports: 7 weeks
- Pivot sports: 13 weeks
- SPN transient paraesthesia (2)
- SPN persistent hypoesthesia (2)
- Persistent instability (1)
Burn et al (2013) [20]
Open modified Broström-Gould
41
- Week 0-4: Cast
- Week 4-8: ankle splint (day + night)
- Week 8-10: ankle splint (only night)
- From day 0: FWB
- From week 5: ankle exercises in sagittal plane
- Week 7: proprioception & coordination training
- One plane sports: 7 weeks
- Pivot sports: 13 weeks
Not stated
Cho et al (2012) [21]
Open modified Broström
40
- Week 0-4: Cast
- After week 4: elastic ankle bandage
- Week 0-4: Non-WB
- Week 5-6: Partial WB
- After week 6: FWB
- From week 4: ROM exercises
- From week 6: peroneal muscle strengthening, proprioception training
- From week 12: running
Not stated
- Wound infection (2)
- SPN damage (1)
- Persistent ankle pain (1)
Li et al (2009) [22]
Open modified Broström
52
- Week 0-4: Cast
- Week 4-6: Ankle Support Orthosis
- Week 0-2: Non-WB
- Week 3-4: increasing to FWB
- From week 4: ROM exercises
- Week 6-8: strengthening & proprioception training
- Week 8-12: plyometrics
16 weeks
- Re-rupture (3)
- Wound infection (several)
Brodsky et al (2005) [23]
Open modified Broström-Gould
73
- Week 0-4: Cast
- After week 4: Walking boot
- Week 0-4: Non-WB
- After week 4: Partial WB – increasing to FWB
- From week 4: Passive dorsi-flexion & plantar flexion
- Week 8: Peroneal muscle strengthening, proprioception & balance training
10-12 weeks
- Superficial ulcer from cast (1)
- Reflex sympathetic dystrophy (1)
- Tibial sesamoiditis (1)
Schmidt et al (2005) [24]
Karlsson procedure
32
- Week 0-3: Cast
- Week 3-6: Air stirrup
- Week 0-3: -
- Week 3-6: FWB
- From day 3: Dorsi-flexion & plantar flexion
- From week 3: Motion, coordination, balance, proprioceptive training
Not stated
- Prolonged wound healing (1)
- Major instability (1)
Jarvela et al (2002) [25]
Karlsson procedure / primary repair
32
- Week 0-4: Cast
- From week 0: FWB
- From week 4: ROM & isometric peroneal strengthening exercises
2-3 months
- Persistent instability (2)
Matsui et al (2016) [26]
Arthroscopic anatomic reconstruction / Open repair
37
- Several days: Compressive bandage and ankle splint
- Up to 6-8 weeks: soft ankle brace
- From day 1: FWB
- From day 1: active ankle ROM†
- Week 1-2: exercises to restore ROM and strength
- Week 2-3: treadmill, sport-specific drills, balance training
6 weeks
- SPN paraesthesia (3)
- Wound irritation (3)
Trichine et al (2018) [27]
Anatomic reconstruction
38
- 45 days: Cast
- 0-15 days: NWB
- 15-30 days: WB
- Week 6: ankle tonification in sagittal plane
- Week 8: coordination, proprioception
- One-plane sports: 8 weeks
- Pivot sports: 14 weeks
- Delay in wound healing (3)
- Transient SPN paraesthesia (2)
Miyamoto et al (2014) [28]
Anatomic Reconstruction using autograft
Group I: 15
Group A: 18Group I
- Week 0-4: Cast
- Week 4-8: Orthosis
Group A
- Week 0-8: Orthosis
Group I
- Week 0-2: Non-WB
- Week 3-4: partial WB
- From week 5: FWB
Group A
- From week 0: FWB
Group I
- From week 4: ROM & strengthening exercises
- Week 6-7: Balance, treadmill, sports drills
Group A
- From week 2: ROM & strengthening exercises
- Week 2-3: Balance, treadmill, sports drills
When patients felt confident and had no difficulties with sports drills
None
Non-anatomic Reconstruction
Ramdass et al (2019) [29]
Anatomic vs non-anatomic reconstruction
An.: 26
Non-An.: 36
- Week 0-4: Cast
- Week 4-8: Ankle boot
- Week 0-4: Non-WB
- Week 4-8: protected WB
- From week 2: ROM exercises
- From week 8-12: physiotherapy
- From week 10-12: protected physical activity
Not stated
- Sural neuroma (1)
- Transient sural neuralgia (1)
- CRPSa (1)
- Ankle arthritis (4)
- Migration of anchor (1)
Benazzo et al (2013) [30]
Non-anatomic reconstruction with fibular periosteal flap
40
- Week 0-6: Cast
- Week 0-3: Non-WB
- From week 3: FWB
- From week 6: ROM exercises
- From Day 50: Proprioception training, muscle strengthening
- From Day 65: Eccentric muscle strengthening
4 months
- Superficial wound infection (1)
Morelli et al (2010) [31]
Modified Watson-Jones
14
- Week 0-4: Cast
- Week 0-2: Non-WB
- From week 2: FWB
- From week 4: ROM exercises
Mean 6 months
- Delay in wound healing (2)
- Transient SPN paraesthesia (3)
*Weight-bearing status abbreviations: FWB (Full Weight-Bearing), WBAT (Weight-Bearing As tolerated), Non-WB (Non-Weight-Bearing)
#SPN: Superficial Peroneal Nerve
8OCL: Osteochondral Lesion
†ROM: Range of Movement
aCRPS: Complex Regional Pain Syndrome
Table 1: Studies providing post-operative rehabilitation protocols (2002–2022) following CLAI surgery.
Rehabilitation protocols for the anatomic repair/reconstruction studies are detailed in table 1 and illustrated in figure 2. Almost 82% of studies immobilized patients in a below knee cast from day 1 post-operatively for two weeks. During the same time, patients were kept non-weight-bearing for the first two weeks in 64% of studies, as seen in figure 3B. 72.7% of protocols suggested keeping the cast for an additional week, and 45.4% for four weeks in total. Only two studies recommended keeping the cast for six weeks in total (9%). There were some studies that placed patients in a walking boot, an elastic brace, or a combination of the two from immediately post-operatively. Overall, a type of boot or brace was kept up to 6 weeks in 82% and 8 weeks in 41% of studies. In terms of full weight-bearing, there were two highlight periods in which authors recommended – at the very start following surgery, on day 1 (32%), or after four weeks from surgery (36%) (Figure 2B).

Figure 2: Bubble plots showing post-operative rehabilitation protocols for anatomic repair or reconstruction of CLAI. Size of the bubble proportional to the number of studies describing the rehabilitation strategy, i.e. the bigger the bubble, the more studies describe the strategy (weeks are shown in the x axis). (a) Immobilisation techniques as described in weeks, (b). Weight-bearing status per week, (c). Rehabilitation, physiotherapy exercises and return to sports.
POP: Plaster Of Paris, NWB: Non-Weight-Bearing, PWB: Partial Weight-Bearing, FWB: Full Weight-Bearing, ROM: Range Of Movement.
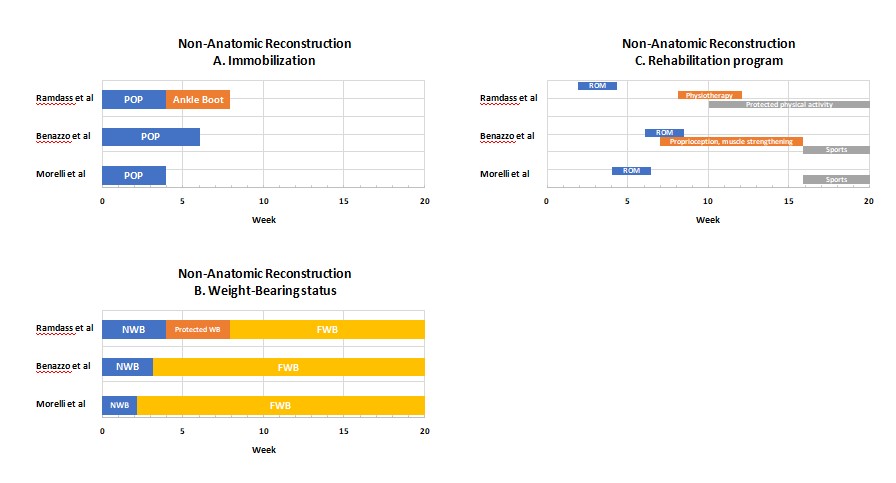
Figure 3: Post-operative rehabilitation strategies for non-anatomic reconstruction of CLAI. (a). Immobilization techniques, (b). Weight-bearing status per week, (c). Rehabilitation and physiotherapy per week (bars and not indicative of length of physiotherapy or exercises, but rather the start).
POP: Plaster Of Paris, NWB: Non-Weight-Bearing, FWB: Full Weight-Bearing, ROM: Range Of Movement.
In terms of exercises allowed, most authors would start range of movement in the sagittal plane after week 2, with muscle strengthening, proprioception, and balance between week 2 and 6, but mostly at week 6 (30%) (Figure 2C). Inversion is usually allowed after week 6. Few studies reported start of different light exercises such as jogging, swimming, and cycling – from the data collected, these can start between weeks 2-6, with more specific sports training after week 6. Return to sports varies considerably between studies and the type of sport and can be anything between 2 and 4 months (Figure 2C).
Rehabilitation protocols for the non-anatomic reconstruction studies are again detailed in table 1 and illustrated in Figure 3. All authors placed their patients in a cast post-operatively for a period of 4-6 weeks and kept them non-weight-bearing between 2-4 weeks (Figure 3A & 3B). Full weight-bearing was then recommended. There was limited information on specific exercises and timing, but range of movement was initiated early usually by week 4 (Figure 3C). Return to sports was suggested from 4 months post-operatively.
Post-operative complications were monitored and are shown in table 2. Three studies did not mention complications, whereas two studies from the anatomic group stated they had no post-operative complications. For the anatomic repair group, the most frequent complications were wound infection (1.7%), and injury to the superficial peroneal nerve which settled within a few months from surgery (1.4%). Ankle instability was reported in 1.5% of cases. For the non-anatomic reconstruction group, ankle arthritis and transient paresthesia along the superficial peroneal nerve were the two most common complications.
Discussion
The ankle is an intricate joint, comprised of the talocrural joint and the tibiofibular syndesmosis, as well as medial and lateral ligamentous complexes that provide static and dynamic stability. Due to the structure of the ankle – the medial malleolus being shorter than the lateral malleolus – the ankle tends to invert, thus making the lateral ligamentous complex more susceptible to injury [32]. The ATFL possess the lowest ultimate load of the three lateral ligaments, which makes it the weakest of the three and thus more likely to be involved in ankle sprains, followed by the CFL [33].
With poor rehabilitation, one in five patients sustaining an ankle sprain will develop chronic instability. There are certain risk factors which can predispose an individual to developing CLAI. Individuals who have a high BMI, generalized ligamentous laxity, females (due to increased laxity of ligaments of the ankle) or those with deformities such as hindfoot varus and midfoot cavus, are at an increased risk [3,5]. Furthermore, athletes who participate in jumping sports such as basketball are also theoretically at risk [34].
Patients with CLAI provide history of inversion injuries and recurrent ankle sprains, often with protected weight bearing [3]. When there is a failure of recovery over a period of 6 weeks and there is mechanical and functional under-performance, it is referred to as chronic ankle instability [35]. Mechanical instability is due to ligament laxity, whereas functional instability is caused by poor posture, neuromuscular and proprioceptive deficits; mechanical and functional instability often overlap [35].
CLAI management can be nonoperative or operative. Patients should ideally be trialed with a minimum of three months of physiotherapy before any operative repair is considered [34]. Although most patients who are managed conservatively will show improvement, those who remain symptomatic for more than six months can be considered for operative repair. The main focus of operative intervention is to improve stability of the ankle joint and to prevent complications including osteoarthritis. Techniques include anatomical repair or reconstruction and non-anatomical reconstruction [6]. The most widely used technique is the one described by Broström in 1964, of suture or transosseous reinsertion of the ATFL and CFL [6]. Since then, many modifications have been described, with or without arthroscopic assistance.
There is no standardized post-operative rehabilitation program following repair or reconstruction for CLAI [36]. Post-operatively, initially there is a period of immobilization which is usually in a cast for anything between 2 and 6 weeks, followed by immobilization in a walking boot, which is also variable. Weight-bearing is again a controversial topic, with some studies suggesting early full weight-bearing, while others advising against it. The restrain from allowing early mobilization and ROM is demonstrated in a systematic review comparing early versus delayed mobilization post-operative protocols for LCL repair [2]. In this study, authors reported higher complication rates and postoperative laxity in the early-mobilized group. However, it was also reported that the post-operative functional outcome, using the AOFAS and Karlsson scores in the early mobilized was improved, making the postoperative laxity finding perhaps not so clinically relevant [2]. The Chinese Society of Sports Medicine has reached a consensus statement, providing clinical guidelines for the operative management of CLCL instability. Among these, they recommend early ROM (mostly dorsiflexion) and partial weightbearing in a brace from day two after surgery, for patients undergoing anatomic repair or reconstruction [37].
From the protocols that were included in this review, more than 80% suggested immobilization in a cast for two weeks with non-weight-bearing. This was then followed usually with a walking boot for four weeks, with initiation of weight-bearing after removal of cast. Patients were started on ROM exercises in the sagittal plane from 15 days following surgery, with inversion allowed after week six. Proprioception and balance exercises were also suggested to start early in the recovery period, between two and six weeks. Depending on the sport, patients were advised to return to sports between two and four months after surgery.
It is very important to understand the basic science of what we are trying to achieve with surgery in CLAI to make correct recommendations in probably an equally important phase of treatment, which is the rehabilitation. Anatomic repair in CLAI aims to restore the bone-ligament interface, a transitional zone which follows Wollf’s law [38]. It is well known that with stress deprivation, mechanical properties of both bone and ligament decrease [39]. Therefore, in order to achieve the optimum repair, some mechanical stimulus is required. If the mechanical environment is not desirable, instead of a bone-ligament transitional zone, there is formation of scar tissue [40].
Neuromuscular rehabilitation is key part of the recovery phase following surgery for CLAI. Both strengthening of the evertor group muscle as well as proprioception exercises are equally important with re-instituting the mechanical properties of the repair. Even with a short period of joint immobilization, functional deconditioning may occur [41]. Therefore, early controlled and supervised ROM is advisable. Proprioceptive training has been a major part of CLAI rehabilitation since Freeman’s publication in 1965 [42]. Its main aim is to reduce symptoms of giving way and reduce function deficits [43].
Based on the evidence presented, the collective presentation of rehabilitation protocols and taking into consideration the evidence-based approach from ESKKA-AFAS Ankle Instability group, the following rehabilitation protocol can be considered after CLAI surgery using anatomic repair (Table 3). In the first two weeks, patients may be immobilized in a cast and non-weight-bearing. After cast removal and inspection of the surgical wound, patients may be placed in a boot and allowed full weight-bearing with the boot on. Patients may be allowed to remove the boot for ROM exercises in the sagittal plane, and light evertor muscle group strengthening exercises may be initiated. If inversion/eversion exercises are to be allowed during this time, these should be supervised and controlled. After six weeks, patients may remove the walking boot and start the early rehabilitation phase, with muscle strengthening exercises of the whole lower limb, proprioception and balance and gait training. During the late rehabilitation phase, between weeks 8-12, the emphasis is on functional, unilateral fully weight-bearing exercises such as plyometrics and jogging. During this phase, functional tests can be used to identify patients ready to progress to the return-to-play phase, usually between 3-4 months post-surgery. Running and sports-specific drills can be started in this phase. Advanced functional tests as well as patients own views on ankle stability should be taken into consideration prior to allowing return-to-sports.
Conclusions
Post-operative rehabilitation protocols following CLAI surgery vary considerably among surgeons. It is very challenging to create a universal rehabilitation protocol based on evidence, simply because very few studies in the literature specifically test their post-operative protocol as their primary outcome measure. With this review article, we attempted to quantify the studies that provide enough information on this subject and create a post-operative rehabilitation protocol following anatomic repair/reconstruction for CLAI, based on basic science and the recommendations given by the ESKKA-AFAS Ankle Instability group. It is clear that this is an area where further high-quality research is required to provide an evidence-based answer.
Author Statements
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- National Institute for Health and Care Excellence (NICE). Sprains and strains; 2020. Available from: https://cks.nice.org.uk/sprains-and-strains#!backgroundSub.
- Vopat ML, Tarakemeh A, Morris B, Hassan M, Garvin P, Zackula R, et al. Early versus delayed mobilization postoperative protocols for lateral ankle ligament repair: A systematic review and meta-analysis. Orthop J Sports Med. 2020; 8: 2325967120925256.
- Al-Mohrej OA, Al-Kenani NS. Chronic ankle instability: current perspectives. Avicenna J Med. 2016; 6: 103-8.
- Tropp H. Commentary: functional ankle instability revisited. J Athl Train. 2002; 37: 512-5.
- Dias S, Lewis TL, Alkhalfan Y, Ahluwalia R, Ray R. Current concepts in the surgical management of chronic ankle lateral ligament instability. J Orthop. 2022; 33: 87-94.
- Tourné Y, Mabit C. Lateral ligament reconstruction procedures for the ankle. Orthop Traumatol Surg Res. 2017; 103: S171-81.
- Teramoto A, Murahashi Y, Takahashi K, Watanabe K, Yamashita T. Effect of accelerated rehabilitation on early return to sport after arthroscopic ankle lateral ligament repair. Orthop J Sports Med. 2022; 10: 23259671221121676.
- Yang KC, Chen PY, Loh C, Tzeng IS, Chang SM, Wang CC. Chronic lateral ankle instability treated with tendon allografting. A preliminary comparison of arthroscopic and open anatomic ligament reconstruction. Orthop J Sports Med. 2022; 10: 23259671221126693.
- Martin KD, Andres NN, Robinson WH. Suture tape augmented Broström procedure and early accelerated rehabilitation. Foot Ankle Int. 2021; 42: 145-50.
- Baraza N, Hardy E, Shahban SA. Reoperation rates following Brostrom repair. JSM Foot Ankle. 2017; 2: 1019.
- Jiang D, Ao YF, Jiao C, Xie X, Chen LX, Guo QW, et al. Concurrent arthroscopic osteochondral lesion treatment and lateral ankle ligament repair has no substantial effect on the outcome of chronic lateral ankle instability. Knee Surg Sports Traumatol Arthrosc. 2018; 26: 3129-34.
- Jeong BO, Kim TY, Song WJ. Effect of preoperative stress radiographic findings on radiographic and clinical outcomes of the modified Brostrom procedure for chronic ankle instability. J Foot Ankle Surg. 2016; 55: 125-8.
- Russo A, Giacchè P, Marcantoni E, Arrighi A, Molfetta L. Treatment of chronic lateral ankle instability using the Broström-Gould procedure in athletes: long-term results. Joints. 2016; 4: 94-7.
- Acevedo JI, Mangone P. Arthroscopic Brostrom technique. Foot Ankle Int. 2015; 36: 465-73.
- Cho BK, Kim YM, Shon HC, Park KJ, Cha JK, Ha YW. A ligament reattachment technique for high-demand athletes with chronic ankle instability. J Foot Ankle Surg. 2015; 54: 7-12.
- Cho BK, Kim YM, Park KJ, Park JK, Kim DK. A prospective outcome and cost-effectiveness comparison between two ligament reattachment techniques using suture anchors for chronic ankle instability. Foot Ankle Int. 2015; 36: 172-9.
- Iwao K, Masataka D, Kohei F. Surgical reconstruction with the remnant ligament improves joint position sense as well as functional ankle instability: A 1-year follow-up study. Sci World J. 2014; 2014: 523902.
- Petrera M, Dwyer T, Theodoropoulos JS, Ogilvie-Harris DJ. Short- to medium-term outcomes after a modified Brostrom repair for lateral ankle instability with immediate postoperative weightbearing. Am J Sports Med. 2014; 42: 1542-8.
- Buerer Y, Winkler M, Burn A, Chopra S, Crevoisier X. Evaluation of a modified Brostrom–Gould procedure for treatment of chronic lateral ankle instability: A retrospective study with critical analysis of outcome scoring. Foot Ankle Surg. 2013; 19: 36-41.
- Burn A, Buerer Y, Chopra S, Winkler M, Crevoisier X. Critical evaluation of outcome scales assessment of lateral ankle ligament reconstruction. Foot Ankle Int. 2013; 34: 995-1005.
- Cho BK, Kim YM, Kim DS, Choi ES, Shon HC, Park KJ. Comparison between suture anchor and transosseous suture for the modified Brostrom procedure. Foot Ankle Int. 2012; 33: 462-8.
- Li X, Lin TJ, Busconi BD. Treatment of chronic lateral ankle instability: a modified Broström technique using three suture anchors. J Orthop Surg Res. 2009; 4: 41.
- Brodsky AR, O’Malley MJ, Bohne WH, Deland JA, Kennedy JG. An analysis of outcome measures following the Brostrom-Gould procedure for chronic lateral ankle instability. Foot Ankle Int. 2005; 26: 816-9.
- Schmidt R, Benesch S, Friemert B, Herbst A, Claes L, Gerngross H. Anatomical repair of lateral ligaments in patients with chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2005; 13: 231-7.
- Järvelä T, Weitz H, Järvelä K, Alavaikko A. A novel reconstruction technique for chronic lateral ankle instability: comparison to primary repair. Int Orthop. 2002; 26: 314-7.
- Matsui K, Takao M, Miyamoto W, Matsushita T. Early recovery after arthroscopic repair compared to open repair of the anterior talofibular ligament for lateral instability of the ankle. Arch Orthop Trauma Surg. 2016; 136: 93-100.
- Trichine F, Friha T, Boukabou A, Belaid L, Bouzidi T, Bouzitouna M. Surgical treatment of chronic lateral ankle instability using an inferior extensor retinaculum flap: A retrospective study. J Foot Ankle Surg. 2018; 57: 226-31.
- Miyamoto W, Takao M, Yamada K, Matsushita T. Accelerated versus traditional rehabilitation after anterior talofibular ligament reconstruction for chronic lateral instability of the ankle in athletes. Am J Sports Med. 2014; 42: 1441-7.
- Ramdass RS, Grierson KR. A comparison of split peroneus Brevis tendon and semitendinosus allograft tendon for lateral ankle ligament reconstruction. J Foot Ankle Surg. 2019; 58: 1197-202.
- Benazzo F, Zanon G, Marullo M, Rossi SM. Lateral ankle instability in high-demand athletes: reconstruction with fibular periosteal flap. Int Orthop. 2013; 37: 1839-44.
- Morelli F, Perugia D, Vadalà A, Serlorenzi P, Ferretti A. Modified Watson-Jones technique for chronic lateral ankle instability in athletes: clinical and radiological mid- to long-term follow-up. Foot Ankle Surg. 2011; 17: 247-51.
- Gibboney MD, Dreyer MA. Lateral ankle instability. Treasure Island, FL: StatPearls Publishing; 2020.
- Fong DT, Chan YY, Mok KM, Yung PS, Chan KM. Understanding acute ankle ligamentous sprain injury in sports. Sports Med Arthrosc Rehabil Ther Technol. 2009; 1: 14.
- Shakked RJ, Karnovsky S, Drakos MC. Operative treatment of lateral ligament instability. Curr Rev Musculoskelet Med. 2017; 10: 113-21.
- Gribble PA, Delahunt E, Bleakley CM, Caulfield B, Docherty CL, Fong DT et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium. J Athl Train. 2014; 49: 121-7.
- Hermanns C, Coda R, Cheema S, Vopat ML, Bechtold M, Tarakemeh A et al. Review of variability in rehabilitation protocols after lateral ankle ligament surgery. Kans J Med. 2020; 13: 152-9.
- Song Y, Li H, Sun C, Zhang J, Gui J, Guo Q et al. Clinical guidelines for the operative management of chronic lateral ankle instability: A consensus reached by systematic review of the available data. Orthop J Sports Med. 2019; 7: 2325967119873852.
- Pearce CJ, Tourné Y, Zellers J, Terrier R, Toschi P, Silbernagel KG, et al. Rehabilitation after anatomical ankle ligament repair or reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016; 24: 1130-9.
- Woo SL, Gomez MA, Sites TJ, Newton PO, Orlando CA, et al. The biomechanical and morphological changes in the medial collateral ligament of the rabbit after immobilization and remobilization. J Bone Joint Am. 1987; 8: 1200-11.
- Galatz LM, Charlton N, Das R, Kim HM, Havlioglu N, Thomopoulos S. Complete removal of load is detrimental to rotator cuff healing. J Shoulder Elbow Surg. 2009; 18: 669-75.
- Fortuna M, Teixeira S, Machado S, Velasques B, Bittencourt J, Peressutti C, et al. Cortical reorganization after hand immobilization: the beta qEEG spectral coherence evidences. PLOS ONE. 2013; 8: e79912.
- Freeman MA. Instability of the foot after injuries to the lateral ligament of the ankle. J Bone Joint Surg Br. 1965; 47: 669-77.
- Rozzi SL, Lephart SM, Sterner R, Kuligowski L. Balance training for persons with functionally unstable ankles. J Orthop Sports Phys Ther. 1999; 29: 478-86.